What happens inside the MCT Kit during each preset is not a passive waiting period. It is a controlled biological conditioning step. In photothermal biomodulation (PTBM), each parameter — wavelength, temperature, fluence, and exposure time — is selected based on its intended biological effect on platelet-rich plasma (PRP), to modulate its biological properties before use as an autologous treatment product.
This is why the MCT System should not be understood simply as a device that exposes autologous whole-blood-derived preparations to light and temperature. Its rationale is more precise: to apply a defined, repeatable chain of physical stimuli to biological material to modulate cellular and extracellular responses.
Light as a biological signal
Photobiomodulation (PBM) is based on the interaction between light and endogenous cellular chromophores. In the red and near-infrared spectrum, mitochondrial cytochrome c oxidase is considered one of the principal photoacceptors, although PBM mechanisms are complex and remain an active field of research.¹ Activation of mitochondrial pathways has been associated with changes in ATP synthesis, reactive oxygen species (ROS) signaling, intracellular calcium modulation, and downstream biological responses that may include growth-factor modulation — processes that can influence cell metabolism, proliferation, and tissue-repair responses.² ³
For regenerative medicine, this is especially relevant because the biological response to PBM depends strongly on the set of parameters used. Wavelength, fluence, irradiance, exposure time, and cell type all matter. This parameter-dependence is particularly important when interpreting PBM studies, since differences in wavelength, fluence, irradiance, exposure time, and cell model can substantially influence the observed biological outcomes.
In 2021, Pinto et al. published a review of in vitro studies using photobiomodulation, photoactivation, or photomodulation in human mesenchymal cells, with wavelengths ranging from 600 to 1000 nm. Of the 42 original articles and five reviews initially identified, 37 studies were selected, covering 43 procedures. The review reported effects on viability, proliferation, differentiation, and migration, concluding that PBM may enhance regenerative capacity when appropriate irradiation parameters are applied.⁴ Although focused on human mesenchymal cells, this review is relevant because it illustrates the parameter-dependent nature of PBM responses.
Temperature as a second biological variable
MCT adds a second controlled variable: temperature. This is important because biological material does not respond to light in isolation. Temperature can influence membrane dynamics, enzymatic activity, platelet behavior, and vesicle-release kinetics. In practice, MCT uses temperature not as a background condition, but as part of the biological stimulus.
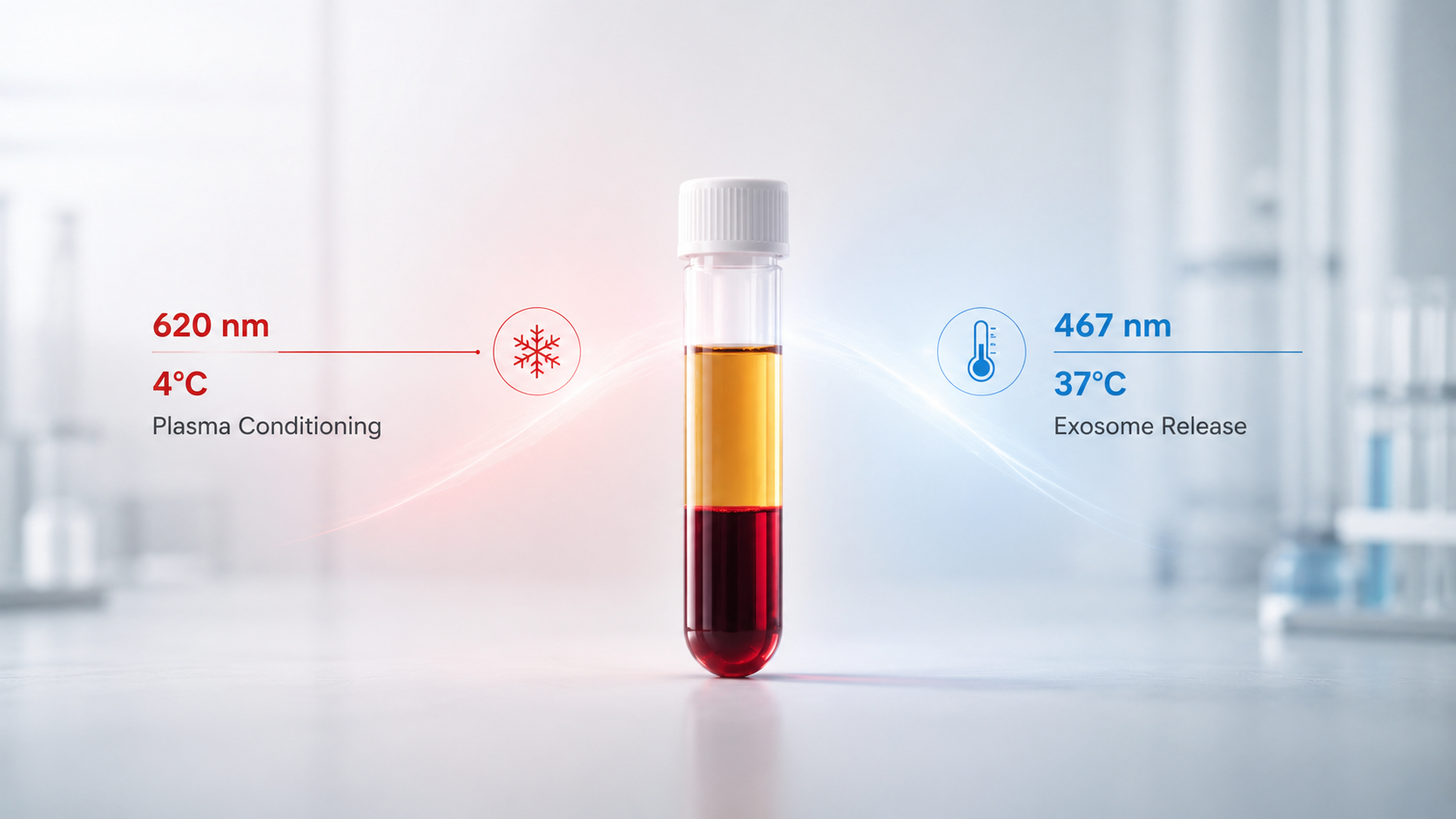
The two MCT protocols reflect this logic. The “PRP” protocol combines 620 nm light with controlled cooling at 4°C. The rationale is platelet priming and modulation of growth-factor and inflammatory signaling pathways. In the “Exosomes” protocol, 467 nm blue light is combined with 37°C, a physiological temperature selected to support platelet-derived extracellular vesicle release during the conditioning phase.
The key concept is that the physician is not applying “light” in general. The physician is applying a protocol: wavelength, temperature, and exposure time, in a defined medical device, for a defined biological objective.
Two protocols, two biological intentions
The “PRP” protocol — 620 nm plus 4°C — is designed for PRP conditioning. The clinical rationale is that PRP is not merely a platelet concentrate; it is a dynamic biological system capable of releasing growth factors, cytokines, and extracellular vesicles.
Clinical evidence has begun to explore this approach. Beltrán and colleagues evaluated the “PRP” preset in the context of photothermal-bioactivated PRP for facial rejuvenation, assessing safety and efficacy compared with previous non-PTBM PRP treatments. The study reported favorable patient- and physician-reported outcomes, with few side effects and no technical drawbacks.⁵ Tejero and colleagues later reported a split-hand comparison in which hands treated with PTBM-PRP tended to show better improvement in subepidermal low-echogenic band reduction than those treated with standard PRP, with patient satisfaction and no technical complications reported.⁶
The “Exosomes” protocol — 467 nm plus 37°C — applies a different logic. Here, the objective is not platelet activation in the conventional sense, but the controlled release of naïve platelet-derived exosomes. In the 2025 in vitro study by Cordero et al., PRP samples from healthy donors were conditioned for ten minutes with blue light at 467 nm and controlled heating at 37°C. The exosomes were isolated by ultracentrifugation and quantified by nanoparticle tracking analysis. The protocol using 1.0 J/cm² produced a mean concentration of 2.99 × 10¹¹ particles/mL, equivalent to approximately 299 × 10⁹ particles/mL.⁷
From empiricism to controlled stimulation
In regenerative medicine, many procedures still depend on a simple sequence: prepare the autologous product, inject it, and observe the clinical response. PTBM introduces a more controlled, parameter-based logic. The biological material is conditioned through documented physical parameters before use.
This is the practical meaning of a controlled stimulus chain. The MCT System combines wavelength, temperature, and time so the clinician can select the targeted biological pathway: platelet priming or exosome release. The value of the platform lies not in adding complexity, but in reducing biological uncertainty.
Photothermal biomodulation is therefore not an accessory feature. It is a systematic approach to autologous biological activation — one in which every parameter is part of the clinical decision.
References
-
Hamblin MR. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochem Photobiol. 2018 Mar;94(2):199-212. doi: 10.1111/php.12864.
-
Maghfour J, Ozog DM, Mineroff J, Jagdeo J, Kohli I, Lim HW. Photobiomodulation CME part I: Overview and mechanism of action. J Am Acad Dermatol. 2024 Nov;91(5):793-802. doi: 10.1016/j.jaad.2023.10.073.
-
Tafur J, Mills PJ. Low-intensity light therapy: exploring the role of redox mechanisms. Photomed Laser Surg. 2008 Aug;26(4):323-8. doi: 10.1089/pho.2007.2184.
-
Pinto H, Goñi Oliver P, Sánchez-Vizcaíno Mengual E. The Effect of Photobiomodulation on Human Mesenchymal Cells: A Literature Review. Aesthetic Plastic Surgery. 2021;45:1826–1842.
-
Beltrán B, Sánchez MAR, Melamed G, Pinto H. Efficacy and safety of photothermal-bioactivated platelet-rich plasma for facial rejuvenation. J Cosmet Dermatol. 2023 Feb;22(2):671-673. doi: 10.1111/jocd.15250.
-
Tejero García P, Mota Antigua S, Ortega Zamorano M, de Lima Monteiro Saraiva RM, Pinto H. Photothermal Biostimulation of Platelet-Rich Plasma Improves Hand Rejuvenation Clinical Outcome: A Pilot Study. Photobiomodul Photomed Laser Surg. 2024 Jun;42(7):473-479. doi: 10.1089/pho.2023.0192.
-
Cordero L, Domingo JC, Sánchez-Vizcaíno Mengual E, Pinto H. Autologous platelet-rich plasma exosome quantification after two thermo-photobiomodulation protocols with different fluences. Journal of Photochemistry and Photobiology. Volume 29, 2025. doi: 10.1016/j.jpap.2025.100267.